A gold mine of information – updated 8 March 2021
The focus in this article is on information and studies which the main stream media do not share with us, helping you to form a balanced opinion. “Truth” can have several sometimes contradicting aspects. Science is based on shifting sands of change and willingness to qestion everything. At a time of a declared global pandemic, this face mask article will hopefully contribute to widen the perspective.
Content on this page below:
• Masks increase Covid Risk • Face Mask Tests • Bacterial Pneumonia • Hypoxia & Hypercapnia? • Surgery Without Masks • Psychological Effects • Legal Aspects • Previous Statements • Face Mask Humour
Face Masks Increase Covid-19 Risk
Finally: the mechanics of droplets spreading wearing face masks and the risk for the wearer are plausibly shown in this article.
“Population studies show that the use of masks either resulted in an increased incidence of COVID-19 or had no impact. None of the examined jurisdictions experienced decreased incidence of COVID-19 after the introduction of mask mandates, except two that had already begun a sharp descent in COVID-19 cases weeks earlier.
Two physical mechanisms are proposed to directly contribute to this finding, based on current available research.
The first is scatter mechanics of dispersed respiratory droplets becoming aerosolized on collision with the mesh of a mask on outward exhalation and then lingering in air.
The second is the pressurized and distant peripheral jets of unfiltered exhaled aerosol from the nozzled edges of a mask. These phenomena result in viral particles lingering longer and traveling farther in airspace from a masked person than exhaled respiratory droplets falling close to the body from the orifices of an unmasked person.
There are also chemical mechanisms for increased COVID-19 cases in masked populations. This is likely due to immune suppression caused by hypoxic and hypercapnic conditions, as well as acidotic, immobilized cilia in the lungs, and reduced skin surface available to sunlight for vitamin D production.
Caution is therefore urged against use of masks among those who wish to reduce the risk, either for themselves or others, of infection with SARS-CoV-2 or COVID-19 disease.” [PDMJ]
“Caution is therefore urged against use of masks among those who wish to reduce the risk, either for themselves or others, of infection with SARS-CoV-2 or COVID-19 disease.” [PDMJ January 2021]
“Dentists are warning about the health issues tied to prolonged use of a mask to stop the spread of the coronavirus. They said dental problems associated with “mask mouth,” including gum disease, could lead to serious complications.”
““Gum disease — or periodontal disease — will eventually lead to strokes and an increased risk of heart attacks,” Marc Sclafani, a dentist and co-founder of One Manhattan Dental, told the New York Post about “mask mouth,” which is increasingly causing inflammation and gum disease among patients. Another dentist and co-founder at One Manhattan Dental, Rob Ramondi, said 50% of his patients are suffering from negative health issues due to mask-wearing.” [Washington Examiner, 7 Aug 2020]
“Research published today in the Journal of Clinical Periodontology,1 the official publication of the European Federation of Periodontology (EFP). The study of more than 500 patients with COVID-19 found that those with gum disease were 3.5 times more likely to be admitted to intensive care, 4.5 times more likely to need a ventilator, and almost nine times more likely to die compared to those without gum disease.” [3 Feb 2021]
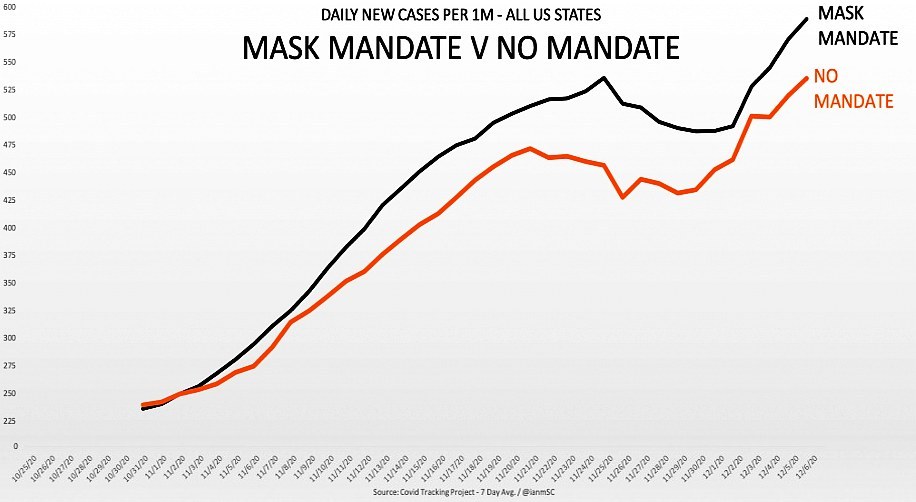
23 Dec 2020: Study: Mask Mandates Increase Rates of COVID Compared to States with No Mask Mandates
“Protective-mask mandates aimed at combating the spread of the CCP virus that causes the disease COVID-19 appear to promote its spread, according to a report from RationalGround.com, a clearinghouse of COVID-19 data trends that’s run by a grassroots group of data analysts, computer scientists, and actuaries. Researchers examined cases covering a 229-day period running from May 1 through Dec. 15 and compared the days in which state governments had imposed mask mandates and the days when they hadn’t. “The reverse correlation between periods of masking and non-masking is remarkable,” RationalGround.com co-founder Justin Hart tweeted on Dec. 20.”
A study of 6,000 Danes was set to reveal whether wearing a face mask actually reduces the risk of COVID-19. The only problem was leading medical journals are refusing to publish the data, and the study’s lead author hinted it’s because they’re not “brave enough” to do it.
“Three medical journals — The Lancet, the New England Journal of Medicine and the Journal of the American Medical Association — have refused to publish the study,” [source in October]
Now PUBLISHED, 18 Nov 2020: “Researchers in Denmark reported on Wednesday that surgical masks did not protect the wearers against infection with the coronavirus in a large randomized clinical trial.”
“Surgical masks did not protect the wearers against infection with the coronavirus in a large randomized clinical trial.”
Roughly 4,860 participants finished the experiment.
42 people in the mask group, or 1.8 percent, got infected,
compared with 53 in the unmasked group, or 2.1 percent.
The difference [0.3%] was not statistically significant.
The study ran from early April to early June 2020. [source]
The Times writes in Sweden claims fall in coronavirus infection rate is down to immunity: “As cases surge across Europe, leading to new restrictions such as the mandatory wearing of masks in many public areas, the infection rate in Sweden is falling. The infection rate in France is more than 60 per cent higher than that of Sweden.”
“France implemented a strict lockdown in the spring and requires masks to be worn in many public areas but has a fortnightly infection rate of 60 cases per 100,000 people.”
“Sweden, which decided not to implement compulsory measures at that time and which rejected the use of masks, has a rate of 37 cases per 100,000 people.”
“Anders Tegnell, the Swedish state epidemiologist leading the response to the pandemic, has noted, based on the statistics, that infection rates have increased in countries such Spain, Belgium and France during and following the mandatory wearing of masks in many public areas. “The belief that masks can solve our problem is very dangerous,”“
This is a strong correlation – however: it does not prove a causation.
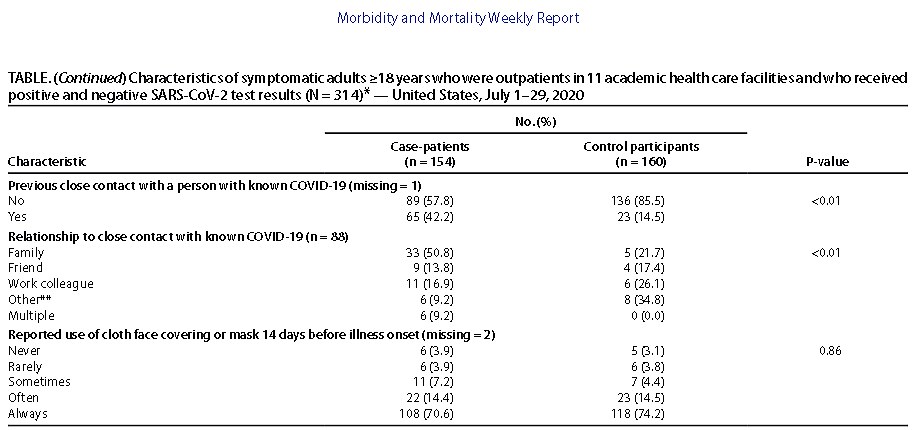
The above table from the CDC study “Community and Close Contact…” shows, that from 154 hospital outpatients with positive covid-19 test results 70% ALWAYS wore a cloth mask – and only 4% never used one.
The control group had similar results. This is an interesting correlation raising questions about health impacts of wearing face masks – however, this does not prove any ‘causation’.
Face Mask Tests
Here is a 53 minute long info video discussing “The Science of Masks” showing that the science can sometimes come to contradicting results.
Below, doctor Ted Noel, an anesthesiologist with 36 years experience wearing different masks in operating rooms explains and shows why masks don’t work – and how the outbreath puffs out sideways and up:



Here is a science summary: Masks Are Neither Effective Nor Safe
Bacterial Pneumonia & Face Masks
UPDATE 24 November: Medical Doctor Warns that “Bacterial Pneumonias Are on the Rise” from Mask Wearing:
Dr. James Meehan, MD followed by warning that mask wearing has “well-known risks that have been well-studied and they’re not being discussed in the risk analysis.”
“I’m seeing patients that have facial rashes, fungal infections, bacterial infections. Reports coming from my colleagues, all over the world, are suggesting that the bacterial pneumonias are on the rise.
“Why might that be? Because untrained members of the public are wearing medical masks, repeatedly… in a non-sterile fashion… They’re becoming contaminated. They’re pulling them off of their car seat, off the rearview mirror, out of their pocket, from their countertop, and they’re reapplying a mask that should be worn fresh and sterile every single time.”
“New research is showing that cloth masks may be increasing the aerosolization of the SARS-COV-2 virus into the environment causing an increased transmission of the disease…”
“In February and March we were told not to wear masks. What changed? The science didn’t change. The politics did.” [source]

As shown in the chapter “Was The Spanish Flu Different?” on HealthTruth.info, viral pneumonia following the influenza spike killed most during the Spanish Flu.
It would be tragic, if the same would happen again in the winter 2020, triggered by excessive face mask wearing.
Skin infections:
Wearing a face mask for a prolongued time can cause skin irritations, known as “maskne” (mask+akne) and is not recommended.

Reminder from the Sydey Morning Herald:
“Farce mask: it’s safe for only 20 minutes“
Retailers who cash in on community fears about SARS by exaggerating the health benefits of surgical masks could face fines of up to $110,000.
NSW Fair Trading Minister Reba Meagher yesterday warned that distributors and traders could be prosecuted if it was suggested the masks offered unrealistic levels of protection from the disease.
“Those masks are only effective so long as they are dry,” said Professor Yvonne Cossart of the Department of Infectious Diseases at the University of Sydney.
“As soon as they become saturated with the moisture in your breath they stop doing their job and pass on the droplets.” [this article is from April 27, 2003 when the world was in a global SARS scare – just like in 2020]

On 12 March 2020 The Independent reported, that one of England’s most senior doctors has warned members of the public they could be putting themselves more at risk from contracting coronavirus by wearing face masks,
Jenny Harries, deputy chief medical officer, said the masks could “actually trap the virus” and cause the person wearing it to breathe it in.
“For the average member of the public walking down a street, it is not a good idea” to wear a face mask in the hope of preventing infection, she added.
Most facemasks contain plastic fibres, which release microparticles when inhaled into the lungs.
Reusable home made and cloth masks need washing; washing powder contains ingredients which may irritate the skin, and the epitelium of the liungs is very sensitive.

A healthy motherly instinct does not need scientific proof to figure this out.

Wearing face masks makes sense in a dusty environment. And they catch droplets when snezing or caughing.
But wearing a mask for a long time can weakens the immune system.
Introducing face masks in the summer, and months after the infections have peaked, was compared to bringing condoms to a baby shower.
Hypoxia & Hypercapnia?
Hypoxia means: there is a reduced amount of oxygen in the blood.
A 2015 study indicated that hypoxia inhibits T-lymphocytes (the main immune cells used to fight infections) by increasing the level of a compound called hypoxia inducible factor-1 (HIF-1). Wearing a mask, which has been shown to cause hypoxia, may actually set the stage for contracting COVID-19 and make the consequences much worse.
Here is a common sense thought:
There’s probably a cup ful of air between the mask and the face of the wearer, containing some outbreath, which gets inhaled on the next breath. Children, old, frail or inactive people with a shallow breath inhale more used air with less oxygen and more CO2. They are more likely to suffer from hypoxia (too little oxygen) or hypercapnia (too much carbon dioxide) in the blood.
This is why children and frail people should NOT wear masks.
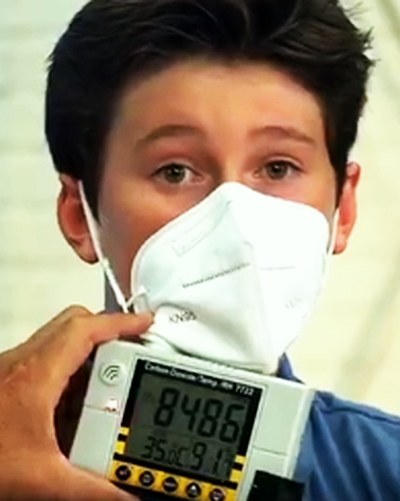
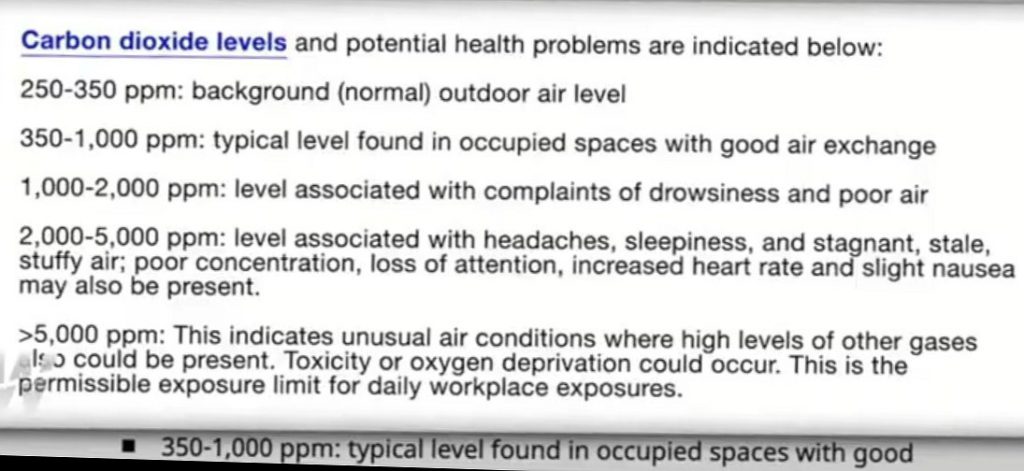
Hypercapnia is an elevated level of CO2 carbon dioxise in the blood. 5000ppm is the limit for safe work places. In the experiment below, the
N95 mask scored over 9999ppm
a blue papermask over 9000ppm
a cloth mask: 9000ppm
a visor / face shield: 1500ppm.
Surgery Without Masks
Dr. Orr’s study: “Is a mask necessary in the operating theatre?“
From March through August 1980, Dr. Orr’s surgeons and staff in the Severalls Surgical Unit in Colchester wore no masks, and compared the rate of surgical wound infections with the rate of wound infections from March through August of the previous four years.
When nobody wore masks during surgeries, the rate of wound infections was less than half what it was when everyone wore masks.
“When nobody wore masks during surgeries,
the rate of wound infections was less than half what it was when everyone wore masks“
Their conclusion:
“It would appear that minimum contamination can best be achieved by not wearing a mask at all” and that wearing a mask during surgery “is a standard procedure that could be abandoned.”
June 2015: Unmasking the surgeons: the evidence base behind the use of facemasks in surgery states:
“While there is a lack of evidence supporting the effectiveness of facemasks, there is similarly a lack of evidence supporting their ineffectiveness.”
“Annual NHS England expenditure on facemasks lies somewhere in the region of £2.5 to £9.1 million.”
The experiment with petridishes shows, that mask use while talking or singing does not make much difference. Unsurprisingly, a sneeze brings out most bacteria, followed by coughing. Nothing new.
Wearing a mask while sneezing or coughing makes sense.
Using a handkerchief (“catch it, bin it“) might probably also do the job.

Psychological Effects of Face Masks
“Masks dehumanize us” Nonverbal Communication in Psychotherapy. “An estimated 60 to 65 percent of interpersonal communication is conveyed via nonverbal behaviors.”
“Masks distort the structure of the face. The lower part of their face is disguised. Identity is concealed. No non-verbal cues or emotion is communicated to a fellow human being can be discerned; all facial communication is hidden under the mask”

First results of a Germany-wide registry on mouth and nose covering (mask) in children:
“Results: By 26.10.2020 the registry had been used by 20,353 people.
In this publication we report the results from the parents, who entered data on a total of 25,930 children.
average wearing time of the mask was 270 minutes per day.
Impairments caused by wearing the mask were reported by 68% of the parents. These included
irritability (60%), headache (53%), difficulty concentrating (50%), less happiness (49%), reluctance to go to school/kindergarten (44%), malaise (42%) impaired learning (38%) and drowsiness or fatigue (37%).“
The psychological effect of signs in shops and other places saying
“You must wear a face mask” can be peceived as intimidating or threatening, especially for those exempted from wearing masks.
Here is an example of a FRIENDLY sign:

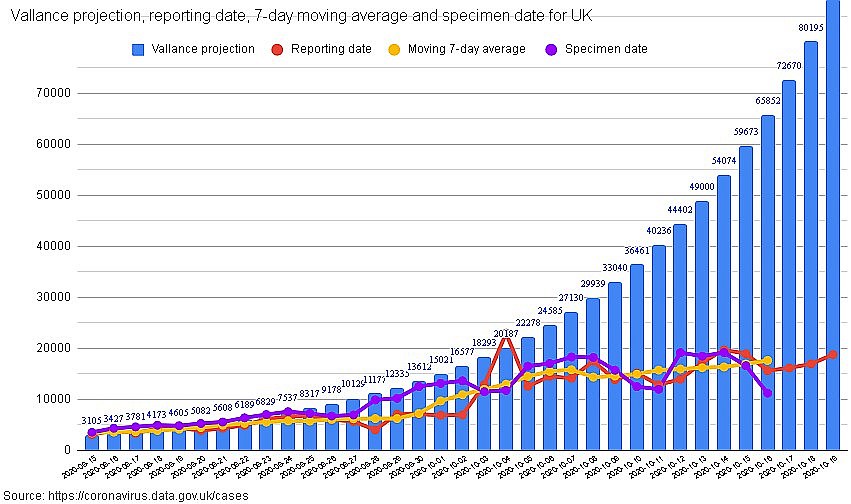
The timing of the introduction to wear face masks in shops in the summer had no scientific foundation – but it kept the fear of the virus alive.
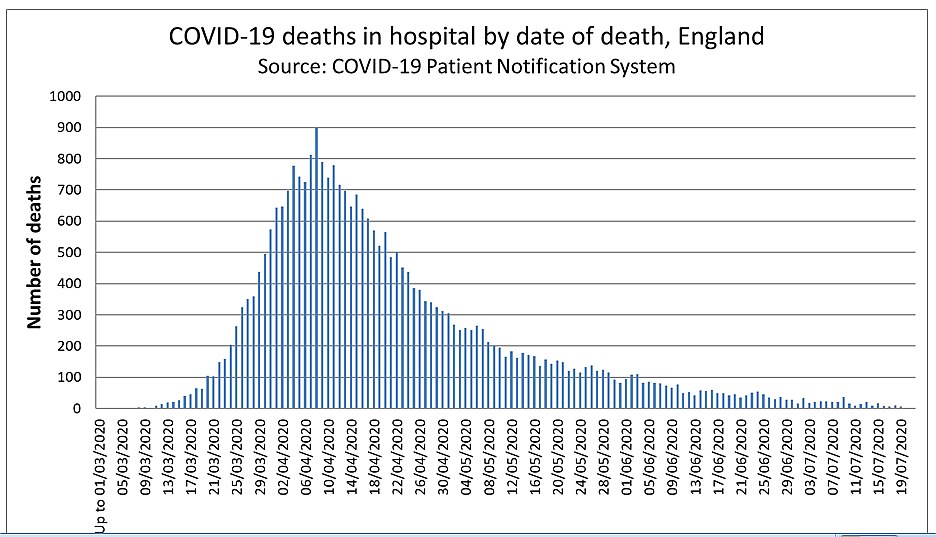
Next year the government might claim “wearing face masks prevented the second wave”? Graphic: NHS England
Legal Aspects & Exemptions
Here is a personal report from Michelle Krinsky:
“Just a little review of my termination in 2018 from a 35 year career in nursing.
I declined the mandatory flu shot. I requested to wear a mask during the duration of “flu season,” which had always been hospital policy.
I was told that surgical masks as well as N95 masks are not effective in filtering viral particulate. Masking was no longer an option and I was fired.”
When you do NOT need to wear a face covering [UK]:
• children under the age of 11
• where putting on, wearing or removing a face covering will cause you severe distress
• if you are undertaking exercise or an activity and it would negatively impact your ability to do so
• to avoid harm or injury, or the risk of harm or injury, to yourself or others
• if you are delivering a sermon or prayer in a place of worship
• if you are aged 11 to 18 attending a faith school and having lessons in a place of worship as part of your core curriculum
[from gov.uk 4 December 2020]
From a Specialist Disability Discrimination Lawyer: Anna de Buisseret IMPORTANT MASK INFORMATION
The Government has FAILED to conduct a Risk Assessment of the risks to the individual members of the public for the harms caused to them by mask wearing– or wearing a face covering.
Without such a Risk Assessment, the individual is NOT providing “informed consent” to wear a “medical device” (which a mask is as defined under the Medical Devices Regulations 2002).
A face “covering” falls to be regulated under the Consumer Protection Regulations. The Face Coverings Regulations are therefore – prima facie – unlawful and should not be enforced.
In the view of our legal team, the Face Coverings Regulations are ultra vires the Government’s powers but that legal argument is ongoing.
None of the supermarkets are providing their customers with a Risk Assessment either – so their customers are also not able to provide their “informed consent” to wearing a face covering /mask.
This is unlawful as “informed consent” must be obtained.
Anyone being asked to wear or use a medical device – such as a mask – should be medically assessed by an Occupational Health team for their INDIVIDUAL risk posed to them by wearing a mask.
Failure to conduct a Health & Safety Risk assessment is both a civil and a potentially criminal offence.
Therefore both the Government and the supermarkets – and anyone else enforcing mask mandates in the absence of a full Health & Safety Risk assessment in the workplace -, is acting unlawfully and can be held PERSONALLY liable for the damage caused to the individual.
Legal challenges are already being run against the “mask perpetrators” to challenge this unlawful and harmful mask mandate and cases are already being won, and damages for harm caused paid out.
I’m a specialist disability discrimination lawyer who also has a stream of claimants lining up to bring legal claims for damages from this mask mandate. Countless people are being harmed by wearing a mask and others are being harmed from the discrimination they are enduring from being mask exempt.
The flood of litigation is going to be Tsunami-like! Be warned: perpetrators will be held to account.
Anyone enforcing or imposing this mandate should be warned that they are acting unlawfully and will be held personally liable for the harm they cause.
I advise anyone harmed by this mask mandate in a work environment (which supermarkets are) to file a report of your harm to the Health & Safety team and ask them to conduct an investigation into whether the employer or supermarket or other “mask perpetrator “ has conducted a valid H&S Risk Assessment.
The local council’s Environmental Health Officer is responsible for ensuring that commercial premises in their area are safe for the public. This includes whether it’s safe for the public to be forced to wear a face covering or mask whilst in a supermarket or other commercial premises. Without a full Risk Assessment, no one should be required or forced to wear a face covering or mask – it’s a breach of the Health & Safety laws and a potentially criminal offence.
If the employer or other “mask perpetrator “ hasn’t followed the law in forcing you to wear a mask, criminal investigations can follow under Health & Safety laws.
The Equality Act 2010 does not permit anyone to discriminate against a disabled person on the grounds of their disability.
Refusing entry to a shop or access to public services to a disabled person is prima facie disability discrimination. No evidence can be lawfully demanded. It’s a breach of both the right to privacy and the Equality Act 2010 to ask for medical evidence in this manner.
Masks worn by the public in community settings, do not prevent transmission of a virus particle as tiny as SARS-CoV-2: that’s what the scientific research evidence shows.
Masks can INCREASE the risk of transmission if not face-fitted and fit-tested for the individual wearer as leakage occurs.
Masks can INCREASE the risk of secondary bacterial and fungal infections due to incorrect putting on and taking off of the mask, incorrect storage and lack of sterilisation of the contamination collecting on the surfaces of the mask.
These contaminates are then inhaled: the moisture and humidity of the mask is a perfect breeding ground for bacteria and fungus which multiply in the mask fibres.
These are then inhaled deeply into the lungs where they multiply further, along with the loose fibres of the mask which collect in the lungs.
Secondary bacterial lung infections are a major risk factor from inhaling bacteria into the lungs. Secondary bacterial lung infections were the major cause of death in the Spanish Flu. They had cloth mask mandates then too. See a correlation?
Masks cause multiple organ damage – some of which is irreparable and permanent.Masks cause social, cognitive, emotional and psychological harm too.
Have YOU been fully informed of all the harms that wearing a mask causes to YOU?
Have YOU had a H&S Risk Assessment by an Occupational Health Team for the risks posed to you – as an individual- for mask wearing? If not, how do YOU know what the risks are? How are YOU providing YOUR individual informed consent to wearing this medical device without a full H&S Risk Assessment? You’re not able to.
You’re simply guessing that it won’t harm you in the absence of a full Risk Assessment.
I have 55 pages of scientific research evidence proving the many harms caused to the mask wearer.
I’ve prepared a detailed Risk Assessment and a Health & Safety Risk Assessment on mask wearing for any of you who would like to be informed of the harms and risks of mask wearing.
There are a team of around 70 of us professional lawyers, medics, Health & Safety inspectors, industrial hygienists, psychologists, scientists and others who are collaborating to raise legal challenges against the unlawful and harmful mask laws and mandates and policies. Our evidence is therefore drawn from top experts in their fields.
4 Sept: a French court rules mandatory masks in public places “serious and illegal infringement” of citizens’ liberties
Some French local authorities are being forced to revise orders making mouth and nose coverings compulsory as courts side with civil liberties groups. A court in Lyon ruled on Friday that making face masks mandatory in all public spaces in Lyon and neighbouring Villeurbanne constituted a “serious and illegal infringement” of citizens’ liberties.
A civil liberty group called “Les Essentialistes” brought the case against authorities arguing that the decrees were disproportionate and inefficient.
The ruling in Lyon followed two similar decisions earlier this week in Strasbourg, in the north-east of France, and in Seine-Maritime, in the north-west.
Mask wearing in the UK is likely to also be challenged in court.
The WHO themselves have been careful to note that they are NOT instructing governments to implement mandatory masks.
If you do NOT wear a mask due to personal reasons and get verbally abused,
“You can claim for the emotional distress the discrimination has caused you – this is called ‘injury to feelings’. You’ll need to say how the discrimination made you feel. Ask your family, friends, medical professionals or support workers if they’ll be witnesses to how the discrimination affected you.”
“You can claim compensation for injury to feelings for almost any discrimination claim. “
“The minimum award for injury to feelings should be around £1,000.” [from citizensadvice.org, England]
It seems, that wearing face masks is solely a political decision.
Please avoid using one way face masks, as they contribute to the contamination of our beautiful planet.
Previous “We Don’t Know” Statements
The WHO states in 2019 “Non-pharmaceuticalpublic health measures for mitigating the risk and impact of epidemic and pandemic influenza“ :
“Face masks worn by asymptomatic people are conditionally recommended in severe epidemics or pandemics, to reduce transmission in the community. Although there is no evidence that this is effective in reducing transmission, there is mechanistic plausibility for the potential effectiveness of this measure.”
The science: Physical interventions to interrupt or reduce the spread of respiratory viruses systematic review and meta-analysis [7 April 2020]:
“Compared to no masks there was no reduction of influenza-like illness (ILI) cases or influenza for masks in the general population, nor in healthcare workers.”
“There was insufficient evidence to provide a recommendation on the use of facial barriers without other measures. We found insufficient evidence for a difference between surgical masks and N95 respirators and limited evidence to support effectiveness of quarantine.”
The WHO writes in a Scientific Brief on 9 July 2020 “Transmission of SARS-CoV-2: implications for infection prevention precautions“:
The physics of exhaled air and flow physics have generated hypotheses about possible mechanisms of SARS-CoV-2 transmission through aerosols.(13-16) These theories suggest that
1) a number of respiratory droplets generate microscopic aerosols (<5 µm) by evaporating, and
2) normal breathing and talking results in exhaled aerosols.
Thus, a susceptible person could inhale aerosols, and could become infected if the aerosols contain the virus in sufficient quantity to cause infection within the recipient. However, the proportion of exhaled droplet nuclei or of respiratory droplets that evaporate to generate aerosols, and the infectious dose of viable SARS-CoV-2 required to cause infection in another person are not known, but it has been studied for other respiratory viruses.(17)
One experimental study quantified the amount of droplets of various sizes that remain airborne during normal speech. However, the authors acknowledge that this relies on the independent action hypothesis, which has not been validated for humans and SARS-CoV-2.(18) Another recent experimental model found that healthy individuals can produce aerosols through coughing and talking (19), and another model suggested high variability between individuals in terms of particle emission rates during speech, with increased rates correlated with increased amplitude of vocalization.(20)
To date, transmission of SARS-CoV-2 by this type of aerosol route has not been demonstrated; much more research is needed given the possible implications of such route of transmission.
Humour & Face Masks:

More about the Immune System


Do women really prefer masked men?

This suggestion by the Terrence Higgins Trust from 10th of August 2020 is ridiculous, and if it is meant to be taken serious, it’s dangerously inhuman. What kind of understanding about the human nature and intimate connections does this show, BBC Newsbeat?
End of this article. Up to top Table of Content