
updated 22 Feb 2021
CONTENT below:
• Intro • What is PCR? • False Positives & Negatives • Cycle Threshold/Amplifications • Peer Review Corman-Drosten Paper • WHO & CDC Update • No Asymptomatic Transmission • Situation @ Universities • PCR Tests Scientifically Meaningless? • Data, Tests & Statistics • Legal Challenges • UK Government? • Antigen & Antibody Tests • Possibilities & Theories
Introduction PCR Test
Polymearase Chain Reaction (PCR) test:
The pcr tests for fragments of the SARS-COV-2 virus,
NOT for the Covid-19 disease.
Healthy people testing “positive” are not “cases”.
A medical “case” has to be ill or show symptoms needing treatment.
To get 100% confirmed real positives, the PCR test must be run at no more than 17 amplification cycles.
Patients cannot be contagious above 25 cycles.
The maximum reasonably reliable Ct value is 30 cycles.
Above 35 cycles, 97% false positives can be expected.
The UK NHS is using up to 45 amplification cycles.
22 international scientists found 10 fatal problems
in the Corman-Drosten paper (basis of the pcr test) and published them in a peer review.
PCR tests are not suitable as specific diagnostic tool.
What Is The PCR Test?
Polymerase Chain Reaction (PCR) is a method widely used to rapidly make millions to billions of copies of a specific DNA sample, allowing scientists to take a very small sample of DNA and amplify it to a large enough amount to study in detail.
A limitation of PCR is that even the smallest amount of contaminating DNA can be amplified, resulting in misleading or ambiguous results.
If you want to dive deeper into the science, read “PCR Amplification“
There is a huge difference between being infected – and being ill.
Healthy people testing positive for coronavirus should not be labelled as “cases”; a “case” has to be ill or show symptoms needing hospital admission. Calling asymptomatic people “a case”,
is medically and psychologically wrong.
Testing infections in a hospital intensive care unit (ICU) brings naturally MUCH higher results than tests including the healthy population (“pillar 2” in the UK). A lot of the same people are being tested once a week, such as nurses and care assistants and people going in to hospitals, so although they may have done say ‘20,000’ tests, that’s 5000 people tested four times each.
“And a word on testing: I do want to emphasize that I’m in the business of testing for Covid. I do want to emphasize that positive test results do not, underlined in neon, mean a clinical infection. It’s simply driving public hysteria and all testing should stop. Unless you’re presenting to hospital with some respiratory problem.”
[23 Nov. Dr. Roger Hodkinson, ex-president of the pathology section of the Medical Association and chairman of a bio technology company in North Carolina selling the COVID-19 test. Full audio is HERE]
A Doctor Reports – from jbhandleyblog.com:
During my career in family medicine, including several years as an Army physician, I have cared for patients with chickenpox, shingles, Lyme disease as well as measles, tuberculosis, malaria, and AIDS.
The “case definition” established for all of these diseases by the CDC requires the presence of signs and symptoms of that disease. Having now been privileged to care for sick patients with COVID-19, both in and out of the hospital setting, I am happy to see the number of these sick patients dwindle almost to zero in my community – while the “case numbers” for COVID-19 continue to go up.
Why is that?
In marked contrast to measles, shingles, and other infectious disease, “cases” of COVID-19 do NOT require the presence of ANY symptoms whatsoever. Health departments are encouraging everyone and anyone to come in for testing, and each positive test is reported as yet another “new” case of COVID-19!
Hence, anyone who has a positive PCR test (the nasal swab, PCR test for COVID Antigen or Nucleic Acid) or serological test (blood test for antibodies –IgG and/or IgM) would be classified as a “case” – even in the absence of symptoms.
In our hospitals at this time, there are hundreds of former nursing home residents sitting in “COVID” units who are in their usual state of good health, banned from returning to their former nursing home residences simply because they have TESTED Positive for COVID-19 during mass testing programs in the nursing homes.
The presence of a positive lab test for COVID-19 in a person who has never been sick is actually GOOD news for that person and for the rest of us.
The positive test indicates that this person has likely mounted an adequate immune response to a small dose of COVID-19 to whom he or she was exposed – naturally (hence, no need for a vaccine vs. COVID-19).
John Thomas Littell, MD, Florida
False Positives & False Negatives
The UK government posted the following study on 3rd of June 2020: “Impact of false-positives and false-negatives in the UK’s COVID-19 RT-PCR testing programme“:
What is the UK operational false positive rate?
“The UK operational false positive rate is unknown… An attempt has been made to estimate the likely false-positive rate of national COVID-19 testing programmes by examining data from published external quality assessments (EQAs) for RT-PCR assays for other RNA viruses carried out between 2004-2019 [7]… giving a median false positive rate of 2.3% (interquartile range 0.8-4.0%).”
“What is the UK operational false negative rate?
The UK operational false negative rate is unknown. A recent study [6] combined results from seven studies… Their model suggested that in the first four days of infection (presymptomatic phase) the probability of a false negative in an infected person decreased from 100% on day 1 (i.e. a false negative was certain) to 67% on day 4.
It then decreased to 38% on day 5 (day of symptom onset) to a minimum of 20% on day 8 of infection.
The false negative rate then increased from day 9 (21%) to day 21 (66%).”
[The “Figure 3” graphic further down illustrates these findings]
Former CSO and VP, Allergy and Respiratory Research Head with Pfizer Global R&D and co-Founder of Ziarco Pharma Ltd., Dr Mike Yeadon writes:
“I have identified a serious, really a fatal flaw in the PCR test used in what is called by the UK Government the Pillar 2 screening – that is, testing many people out in their communities… the Health Secretary, Matt Hancock, misled the House of Commons and also made misleading statements”
Dr Mike Yeadon explains, that a pcr test with 0.8% false positive results means, that 89-94% of pcr “cases” are FALSE positives, as only about 0.1% of the population have coronavirus.
Dr. Wolfgang Wodard: “How can a test that turns out positive for the many different SARS viruses of bats, dogs, tigers, lions, domestic cats and humans, which have been changing and spreading worldwide for many years, be called specific for the detection of an allegedly only four-month-old SARS-CoV-2?”
“The test seemingly also measures earlier SARS variants that are constantly altering, can change hosts quickly and are not found in virologists’ databases. However, these were and are obviously not considered to be extraordinarily dangerous.”
Cycle Threshold/Amplifications
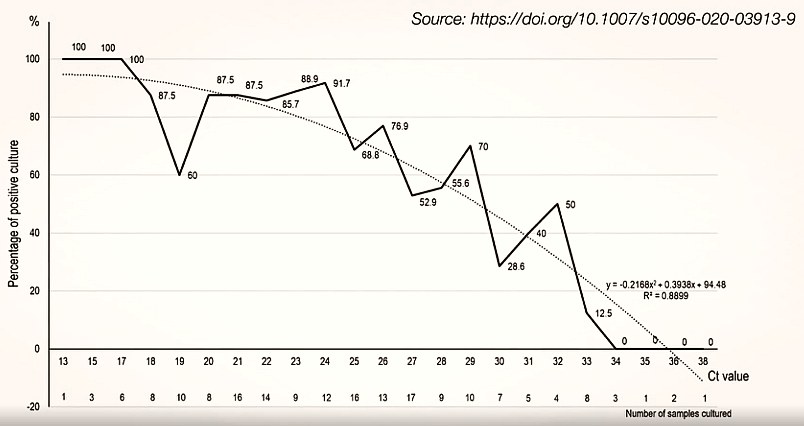
According to an April 2020 study in the European Journal of Clinical Microbiology & Infectious Diseases, to get 100% confirmed real positives, the PCR test must be run at no more than 17 amplification cycles.
Bullard et al reported that patients could not be contagious with PCR Cycle threshold Ct >25 as the virus is not detected in culture above this value.
[this means: if you don’t find a positive virus test result with 25 cycles / amplifications, there is no point increasing the cycles any further]
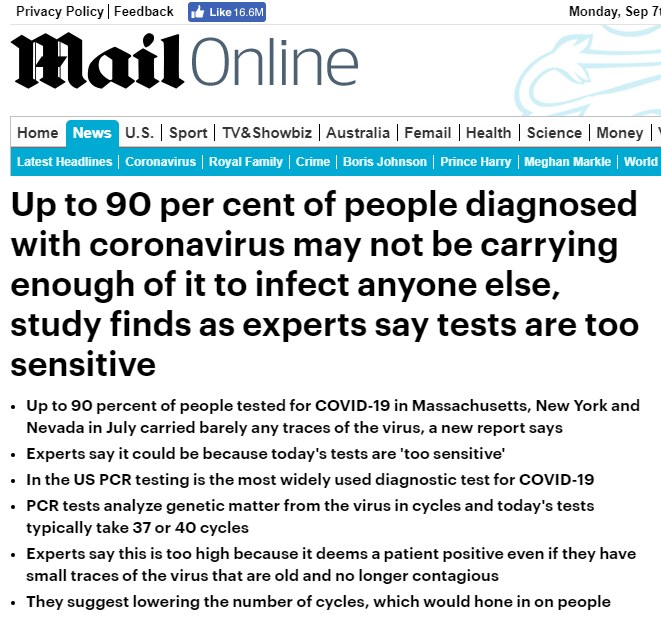
“The threshold value cutoff for the CDC’s PCR test is 40 cycles [of amplifications], a value that many medical experts believe returns false positives, as fragments of a killed virus may be picked up….
What the Cycle threshold [Ct] cutoff value should be varies in discussions among the scientific community, but generally ranges between 25 and 30 with agreement that patients cannot be contagious above these numbers.“
Another viral culture study… reported that patients with threshold values at 34 or above did not “excrete infectious viral particles.”
““We know that after about one week of infection from SARS-CoV-2, people are no longer infectious to others, but they still will be positive with PCR testing because they’ll still have bits of the virus within their body.”
[from: COVID Test Scam: Cycle Threshold Values Being Deliberately Omitted]
“Research by experts at Oxford University suggests as many as half of the “positive” tests relied upon could actually be false because the current test is so sensitive it can pick up dead and harmless viral particles that are shed once the infection has passed.”
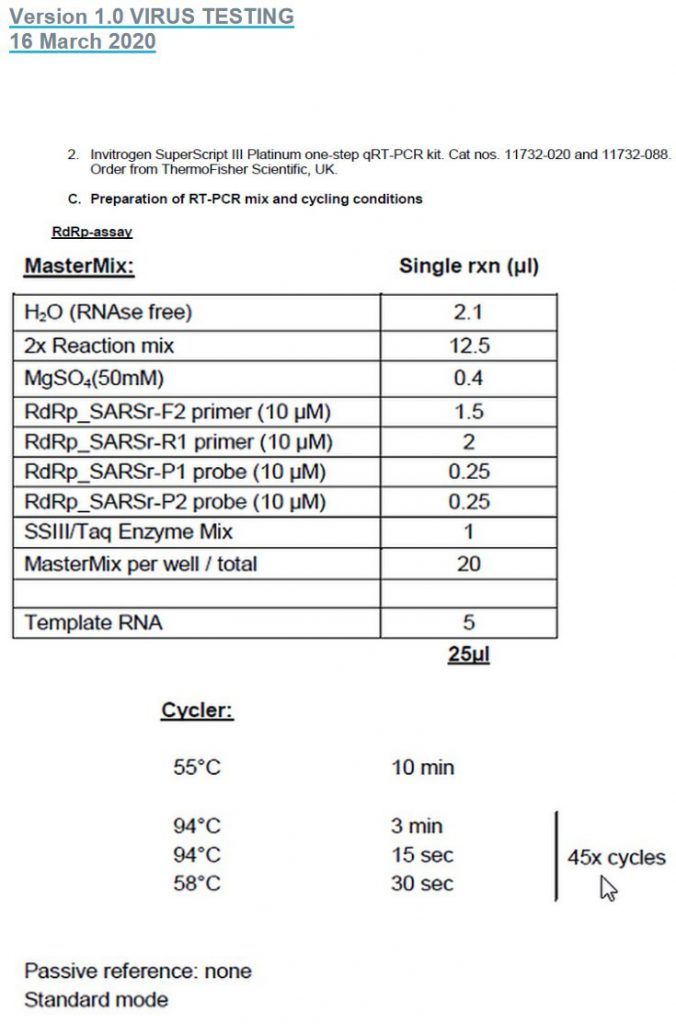
The NHS / UK is using 45 cycle amplifications
in the PCR test:
Here is a short video explaining this
“The PCR swabs take one or two sequences of a molecule that are invisible to the human eye and therefore need to be amplified in many cycles to make it visible. Everything over 35 cycles is, as reported by The NewYork Times and others, considered completely unreliable and scientifically unjustifiable. However, the Drosten test, as well as the WHO recommended tests that followed his example, are set to 45 cycles.”
“The test cannot distinguish inactive and reproductive matter. That means that a positive result may happen because the test detects, for example, a piece of debris, a fragment of a molecule which may signal nothing else, then that the immune system of the person tested won a battle with a common cold in the past.” [‘from Crimes against humanity‘]
“The maximum reasonably reliable Ct value is 30 cycles.
Above a Ct of 35 cycles, rapidly increasing numbers of
false positives must be expected.“
“only non-infectious (dead) viruses are detected with Ct values of 35.” [CORMAN-DROSTEN REVIEW REPORT]
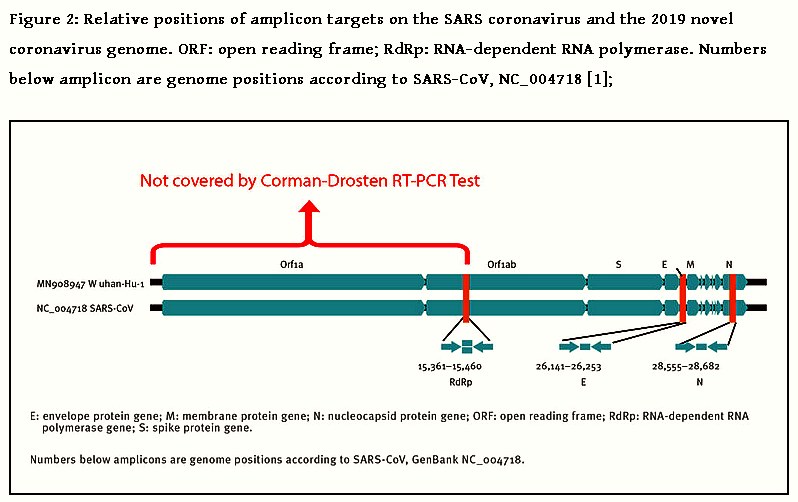
Peer Review Corman-Drosten Paper
On 27th of November, 22 scientists published:
“External peer review of the RTPCR test to detect SARS-CoV-2 reveals 10 major scientific flaws at the molecular and methodological level: consequences for false positive results“
“There are ten fatal problems with the Corman-Drosten paper”
“The published RT-qPCR protocol for detection and diagnostics of 2019-nCoV and the manuscript suffer from numerous technical and scientific errors, including insufficient primer design, a problematic and insufficient RT-qPCR protocol, and the absence of an accurate test validation.
Neither the presented test nor the manuscript itself fulfils the requirements for an acceptable scientific publication.”
This has huge world wide implications, as the WHO-protocol directly derives from the Corman-Drosten paper.
“Further, serious conflicts of interest of the authors are not mentioned. Finally, the very short timescale between submission and acceptance of the publication (24 hours) signifies that a systematic peer review process was either not performed here, or of problematic poor quality.”
We provide compelling evidence of several scientific inadequacies, errors and flaws.
“Considering the scientific and methodological blemishes presented here, we are confident that the editorial board of Eurosurveillance has no other choice but to retract the publication.”
[from Review report Corman-Drosten et al. Eurosurveillance 2020, 27 November]
The CORMAN-DROSTEN REVIEW REPORT continues:
“In case of virus detection, >35 cycles only detects signals which do not correlate with infectious virus as determined by isolation in cell culture [reviewed in 2]; if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the case in most laboratories in Europe & the US), the probability that said person is actually infected is less than 3%, the probability that said result is a false positive is 97%“
“There exists no specified reason to use these extremely high concentrations of primers in this protocol. Rather, these concentrations lead to increased unspecific binding and PCR product amplification.
“The design variations will inevitably lead to results that are not even SARS CoV-2 related. Therefore, the confusing unspecific description in the Corman-Drosten paper is not suitable as a Standard Operational Protocol.
“…in nearly all test procedures worldwide, merely 2 primer matches were used instead of all three. This oversight renders the entire test-protocol useless with regards to delivering accurate test-results of real significance.
“A better primer design would have terminal primers on both ends of the viral genome. This is because the whole viral genome would be covered and three positive signals can better discriminate between a complete (and thus potentially infectious) virus and fragmented viral genomes (without infectious potency).
The CORMAN-DROSTEN REVIEW REPORT continues:
[All three primers have GC values BELOW the 40% minimum (28% 31% and 34.6%)]
“If the Tm-value is very low, as observed for all wobbly-variants of the RdRp reverse primers, the primers can bind non-specifically to several targets, decreasing specificity and increasing potential false positive results.”
A maximal Tm difference of 2° C within primer pairs was considered acceptable. Testing the primer pairs specified in the Corman-Drosten paper, we observed a difference of 10° C …
This is a very serious error and makes the protocol useless as a specific diagnostic tool.
“…the dNTPs (0.4uM) are 2x higher than recommended for a highly specific amplification“
“The design errors described here are so severe that it is highly unlikely that specific amplification of SARS-CoV-2 genetic material will occur using the protocol of the Corman-Drosten paper.“
“…the case of small fragments of qPCR (around 100bp):
It could be either 1,5% agarose gel or even an acrylamide gel.”
“The fact that these PCR products have not been validated at molecular level is another striking error of the protocol, making any test based upon it useless as a specific diagnostic tool to identify the SARS-CoV-2 virus.“
“the functionality of the published RT-PCR Test was not demonstrated with the use of a positive control (isolated SARS-CoV-2 RNA) which is an essential scientific gold standard.”
“the E gene used in RT-PCR test, as described in the Corman-Drosten paper, is not specific to SARS-CoV-2.“
“The E gene primers also detect a broad spectrum of other SARS viruses.
The genome of the coronavirus is the largest of all RNA viruses that infect humans and they all have a very similar molecular structure.
Still, SARS-CoV1 and SARS-CoV-2 have two highly specific genetic fingerprints, which set them apart from the other coronaviruses.
First, a unique fingerprint-sequence (KTFPPTEPKKDKKKK) is present in the N-protein of SARS-CoV and SARS-CoV-2 [13,14,15]. Second, both SARS-CoV1 and SARS-CoV2 do not contain the HE protein, whereas all other coronaviruses possess this gene [13, 14].
In order to specifically detect a SARS-CoV1 and SARS-CoV-2 PCR product the above region in the N gene should have been chosen as the amplification target.
A reliable diagnostic test should focus on this specific region in the N gene as a confirmatory test. The PCR for this N gene was not further validated nor recommended as a test gene by the Drosten-Corman paper, because of being “not so sensitive” with the SARS-CoV original probe [1].”
“The Corman-Drosten paper does not contain this [the HE gene] negative control, nor does it contain any other negative controls. The PCR test in the Corman-Drosten paper therefore contains neither a unique positive control nor a negative control to exclude the presence of other coronaviruses. This is another major design flaw“
“There should be a Standard Operational Procedure (SOP) available, which unequivocally specifies the above parameters, so that all laboratories are able to set up the identical same test conditions. To have a validated universal SOP is essential, because it facilitates data comparison within and between countries. It is very important to specify all primer parameters unequivocally. We note that this has not been done... The protocol as described is unfortunately very vague and erroneous in its design“
“It is inevitable that this test will generate a tremendous number of so-called “false positives”.”
“The Corman-Drosten paper was not peer-reviewed“
“two authors of the Corman-Drosten paper, Christian Drosten and Chantal Reusken, are also members of the editorial board of this journal [19]. Hence there is a severe conflict of interest” [source]
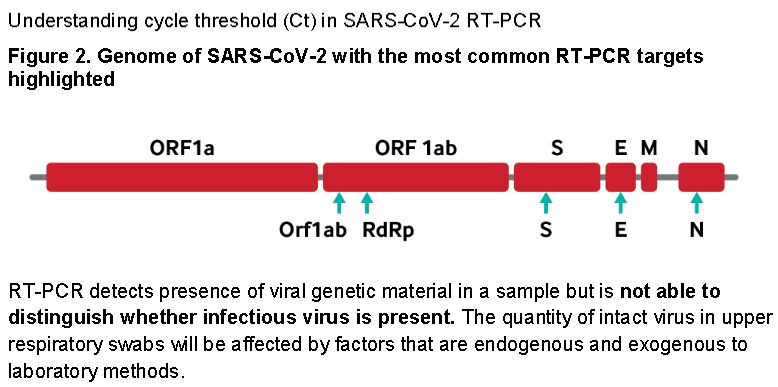
Understanding cycle threshold (Ct) in SARS-CoV-2 RT-PCR: a guide for health protection teams [by gov.uk, 28 October]
“Cycle threshold (Ct) is a semi-quantitative value that can broadly categorise the concentration of viral genetic material in a patient sample following testing by RT PCR as low, medium or high –that is, it tells us approximately how much viral genetic material is in the sample.
A low Ct indicates a high concentration of viral genetic material, which is typically associated with high risk of infectivity.
A high Ct indicates a low concentration of viral genetic material which is typically associated with a lower risk of infectivity.
In the context of an upper respiratory tract sample a high Ct may also represent scenarios where a higher risk of infection remains –for example, early infection, inadequately collected or degraded sample.
The cycle threshold (Ct) can be defined as the thermal cycle number at which the fluorescent signal exceeds that of the background and thus passes the threshold for positivity (Figure 1, page 5).”
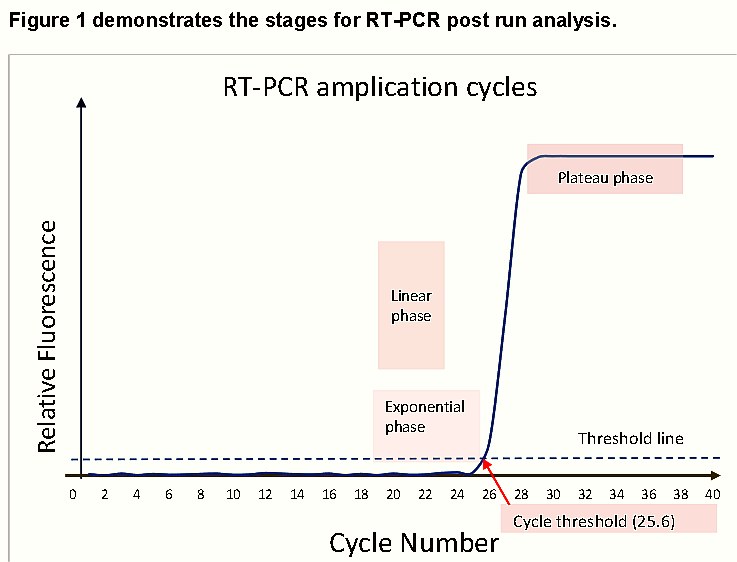
gov.uk continues: “A typical RT-PCR assay will have a maximum of 40 thermal cycles… A 3-point increase in Ct value is roughly equivalent to a 10-fold decrease in the quantity of viral genetic material [in the sample].”
Ct values cannot be directly compared between assays of different types due to variation in the sensitivity (limit of detection), chemistry of reagents, gene targets, cycle parameters, analytical interpretive methods, sample preparation and extraction techniques.
Additionally, Ct values are not provided for all SARS-CoV-2 molecular detection methods. Some commercial RT-PCR techniques are closed ‘black box’systems whereby the operator cannot observe the reaction in real-time and the result is interpreted by software into a qualitative non-interrogatable positive or negative result. [gov.uk]
“A single Ct [Cycle threshold] value in the absence of clinical context cannot be relied upon for decision making about a person’s infectivity.
There are many different SARS-CoV-2 RT-PCR assays/platforms in use across the UK. Ct values cannot be directly compared between assays of different types – not all laboratories use the same assay, and some may use more than one.” [gov.uk]
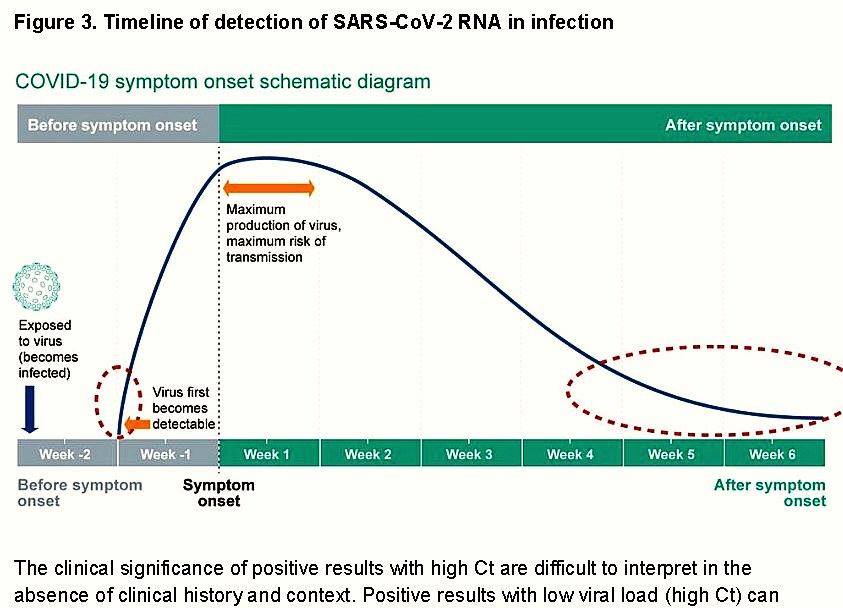
“Positive results with low viral load (high Ct) can be seen in the early stages of infection (before the person becomes capable of transmission of the infection) or late in infection when the risk of transmission is low (periods indicated by the dotted red line).
Recovery phase of infection with diminishing viral load.
Prolonged detection of viral genetic material that is likely to be non-infectious has been observed for SARS-CoV-2.” [gov.uk]
[bold highlighted by HealthTruth.info]
WHO Update PCR Users
WHO UPDATE re. PCR Tests from 20 January 2021:
It seems like the criticism (see more in this chapter) about the number of pcr test amplifications / cycle threshold and the big number of false positve test results has forced the WHO to send out the following NOTICE:
WHO Information Notice for IVD Users 2020/05
Product type: Nucleic acid testing (NAT) technologies that use polymerase chain reaction (PCR) for detection of SARS-CoV-2
Target audience: laboratory professionals and users of IVDs.
Purpose of this notice: clarify information previously provided by WHO. This notice supersedes WHO Information Notice for In Vitro Diagnostic Medical Device (IVD) Users 2020/05 version 1, issued 14 December 2020.
Description of the problem: WHO requests users to follow the instructions for use (IFU) when interpreting results for specimens tested using PCR methodology.
Users of IVDs must read and follow the IFU carefully to determine if manual adjustment of the PCR positivity threshold is recommended by the manufacturer.
WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak positive results is needed (1). The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient’s viral load. Where test results do not correspond with the clinical presentation, a new specimen should be taken and retested using the same or different NAT technology.
WHO reminds IVD users that disease prevalence alters the predictive value of test results; as disease prevalence decreases, the risk of false positive increases (2). This means that the probability that a person who has a positive result (SARS-CoV-2 detected) is truly infected with SARS-CoV-2 decreases as prevalence decreases, irrespective of the claimed specificity.
Most PCR assays are indicated as an aid for diagnosis, therefore, health care providers must consider any result in combination with timing of sampling, specimen type, assay specifics, clinical observations, patient history, confirmed status of any contacts, and epidemiological information.
Actions to be taken by In Vitro Diagnostic Medical Device (IVD) users:
…4. Provide the Ct value in the report to the requesting health care provider.
The US CDC published the following instructions after being criticised:
CDC 2019-Novel Coronavirus (2019-nCoV)
Real-Time RT-PCR Diagnostic Panel
For Emergency Use Only [1 Dec 2020]
Instructions for Use Catalog # 2019-nCoVEUA-01
– – – Quotes from page 38 – – –
• Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms.
• The performance of this test has not been established for monitoring treatment of 2019-nCoV infection.
• This test cannot rule out diseases caused by other bacterial or viral pathogens.
No Asymptomatic Transmission
A peer reviewed article in Nature.com (20 November) looking at PCR test data from nearly 10 million residents in Wuhan city found that not a single one of those who had been in close contact with an asymptomatic individual tested positive
Of the 34,424 residents with a history of COVID-19, 107 individuals tested positive a second time, but none were symptomatic and none were infectious.
This research paper also indicates that “virulence of SARS-CoV-2 virus may be weakening over time“
[summarised by Dr. Mercola 4 Dec & The Last refuge 20 Dec. – read more about Natural Immunity after covid-19]
HealthTruth.info comment:
Without asymptomatic transmissions, all of the current lock-down regulations, mask wearing requirements and social distancing rules have no scientific basis, and could be challenged in court.
Dr Michael Yeadon @MichaelYeadon3, 21 Nov. on Twitter:
“The first time the notion of “asymptomatic transmission” was mentioned, I smelled a rat. It’s biologically implausible. Not saying it’s never happened once, but as an important contribution to transmission? No. To be a source, you need lots of virus in your airway. But once that happens, you will be symptomatic, either because the virus is injuring your lung lining (epithelium) or because you’re fighting it off (or both). You can’t be both a virulent source AND not have symptoms.
Yet it was on the basis that you often wouldn’t show symptoms yet place others at risk that MASS TESTING, all the time, in ever-increasing numbers, was commenced. Now we formally know what basic biology and immunology told us, we can HALT MASS TESTING OF THE ASYMPTOMATIC. We’ve said it for months.
Mr Hancock, stop it now.”
“Asymptomatic transmission”…
To be a source, you need lots of virus in your airway. Once that happens, you will be symptomatic. You can’t be both a virulent source AND not have symptoms.
[Dr Michael Yeadon]
The Situation @ Universities
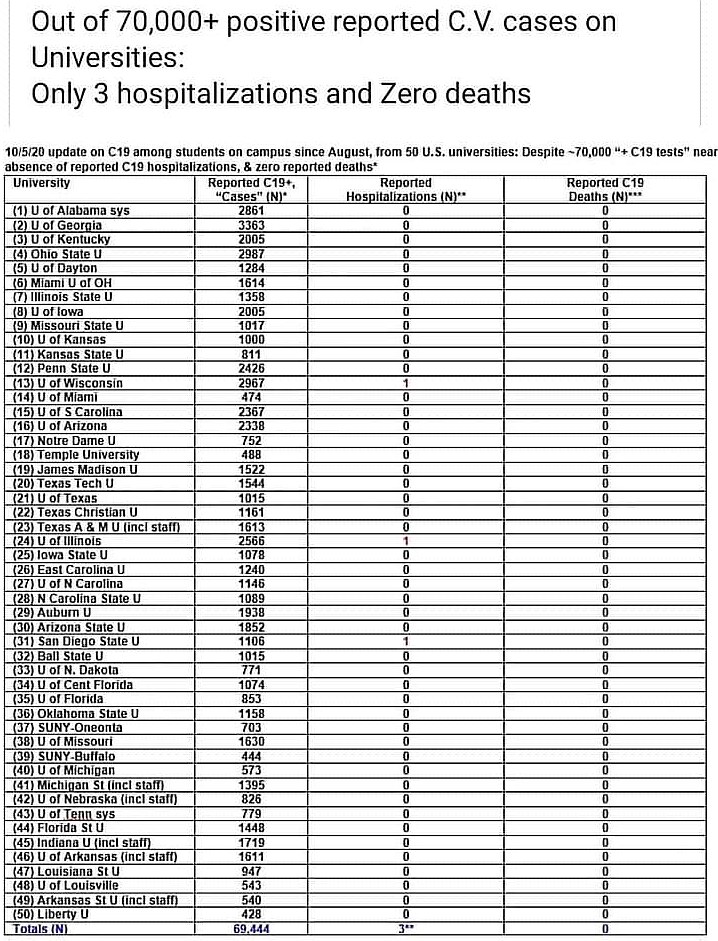
3 real cases, and 69.441 FALSE positive “cases” among students.
Why are students forced to self-isolate, based on PCR tests???
6 December: “All 31 Colleges of the University of Cambridge [UK], and 6 Houses of the Cambridge Theological Federation, participated in the programme. Based on these data, we did not detect any new cases of asymptomatic COVID-19 amongst 9,376 students living in College accommodation screened this week.” [source]
[10 tests were originally positive, but were all found to be “false positives” after confirmatory tests.] See table below.
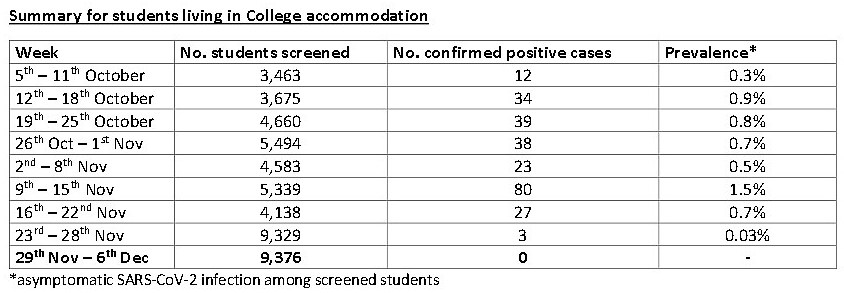
Week 9 (30th November – 6th December 2020) Cambridge University: 0 cases
HealthTruth.info comment: Could this be the end of the pandemic? Due to mingling and mixing at university, a healthy natural immunity is likely to have been aquired among the students.
PCR Tests Scientifically Meaningless?
This OFF-Guardian research article COVID19 PCR Tests are Scientifically Meaningless, digs deep into the science, and painstakingly shows why we should not use these tests or even base a lockdown decisions on them.
PCR is extremely sensitive, which means it can detect even the smallest pieces of DNA or RNA — but it cannot determine where these particles came from. None of the science teams of the relevant papers which are referred to in the context of SARS-CoV-2 for proof could confirm the electron-microscopic shots depicted in their in vitro experiments show purified viruses.
“sleek polymerase chain reaction… tells little or nothing about how a virus multiplies, which animals carry it, [or] how it makes people sick. [It is] like trying to say whether somebody has bad breath by looking at his fingerprint.”
There is no scientific proof that those RNA sequences are the causative agent of … COVID-19, and there are no distinctive specific symptoms for COVID-19.
“Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV is the causative agent for clinical symptoms” [CDC RT-PCR Diagnostic Panel]
Many PCR tests have a “cycle quantification” (Cq) value of over 35.
If you are looking for presumed RNA viruses such as SARS-CoV-2, the RNA must be converted to complementary cDNA with the enzyme Reverse Transcriptase—hence the “RT” at the beginning of “PCR” or “qPCR.” But this transformation process is widely recognised as inefficient and variable, as the amount of DNA obtained with the same RNA base material can vary widely, even by a factor of 10.
On 7 July 2020, Politifact published a “fact check” response to this article, claiming the article is ‘inaccurate’, without contacting either OffGuardian or the authors for comment. Here is the Open Letter: Refuting Politifact’s “fact check” by Torsten Engelbrecht.
Data, Tests & Statistics
COVID cases in England aren’t rising: here’s why
by Carl Heneghan, Centre for Evidence-Based Medicine 2 Aug 2020:
“The government has restricted movements on millions of people in England: COVID is apparently on the rise. But what happens when you start digging into the data. I have used the following data sets to piece together the number of tests, cases and results for Pillar 1* (done in healthcare settings) and Pillar 2* (tests are done in the community)”
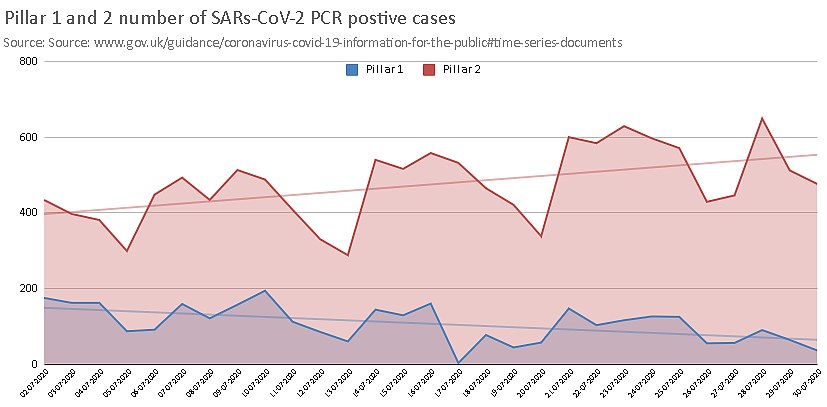
On first glance it looks like the number of cases in Pillar 2 is trending up and Pillar 1 is trending down. This would suggest that the increase in hospitals – in the sickest (Pillar 1) – is staying the same; while in the community Pillar 2 testing is picking up milder asymptomatic disease.
By the 31st July, the Pillar, 1 seven day average for testing had increased to 49,543 (a 20% increase); while the Pillar 2 had risen by much more – by 82% to 78,522 tests.
“The next graph shows what happens when you adjust for the number of tests done and then standardise to per 100,000 tests. Pillar 1 is seen to be still trending down, but Pillar 2 is now flatlining. The increase in the number of cases detected, therefore, is likely due to the increase in testing in Pillar 2.”
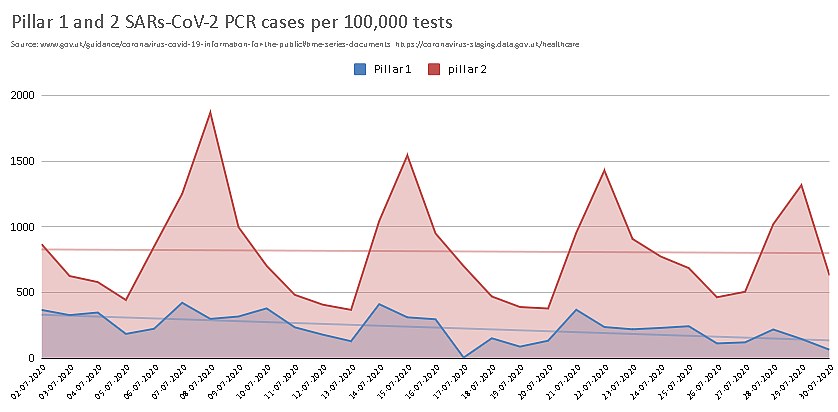
“Inaccuracies in the data and poor interpretation will often lead to errors in decisions about imposing restrictions”
[Carl Heneghan]
The same situation in the US:
“the sudden jump in cases in February correlates with the emergence of test kits sent out by the CDC. Once those test kits were used up, the number of “cases” again dried up. Then, once test kits became readily available again in early April, the number of cases skyrocketed — as you’d expect. But again, this doesn’t mean the disease was spreading like wildfire….Increased Testing = Increased ‘Cases’“
19 October: Patrick Vallance, the Chief Scientist, said: ‘At the moment we think that the epidemic is doubling roughly every seven days.”
Vallance said “If, and that’s quite a big if, but if that continues unabated… you would end up with something like 50,000 cases in the middle of October per day.”
The Centre for Evidence-Based Medicine in Oxford put the doubling to the test by creating a tracker of the projection.
“At the moment there is a significant divergence in the case data”.
Did we not learn from prof Neil Ferguson to distrust mathematical projections? Still they are used to terrify us and justify lockdown.
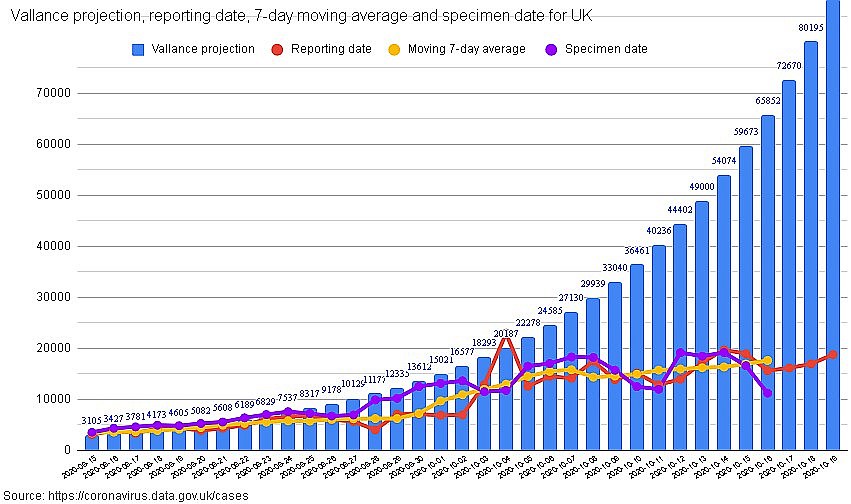
“Tracking UK Covid-19 Cases” data until 19 October
The media focussed on reporting the (green) predictions, but not the real tested “cases”.
Legal PCR Test Challenges
Update 28 Nov: Portuguese Court Rules PCR Tests “Unreliable” & Quarantines “Unlawful” [Nov 11]
“An appeals court in Portugal has ruled that the PCR process is not a reliable test for Sars-Cov-2, and therefore any enforced quarantine based on those test results is unlawful.
Further, the ruling suggested that any forced quarantine applied to healthy people could be a violation of their fundamental right to liberty.“
“Most importantly, the judges ruled that a single positive PCR test cannot be used as an effective diagnosis of infection.”
“The ruling goes on to conclude that, based on the science they read, any PCR test using over 25 cycles is totally unreliable.”
THIS court ruling, based on THIS STUDY, has huge implications for other countries, and was ignored in the main stream media.
[Read more above: “Review report Corman-Drosten”]
More legal update info on “Can the Law Save Us?“
And The UK Government?
Does the UK government take notice of the above findings?
The British Government ordered over three million of test kits from China in spring, and found they are not useable.
In August they called back 750 000 PCR test kits as faulty. They seem to be spending and wasting vast amounts of money towards big companies.
What are these pcr tests good for?
Dept. of Health information
Despite the faults and problems of the PCR test, the UK government decided to spend more money on this project:
Critics have already rounded on the plans as “devoid of any contribution from scientists, clinicians, and public health and testing and screening experts,” and “disregarding the enormous problems with the existing testing and tracing programmes.”
Antigen Tests & Antibody Tests
What is an ANTIGEN Test?
An antigen test is a diagnostic test that checks to see if you’re infected with the coronavirus. The test looks for proteins (antigens) in a sample taken from your nose or throat. Antigen tests are faster than PCR tests, but they have a higher risk of false positives (meaning that they’re more likely to say you have the infection when you don’t). This may also be called a rapid test or rapid diagnostic test. [webmd.com]
Health.com writes:
“An antigen is a substance recognized by the body’s immune system, which can [then] respond by generating proteins called antibodies that specifically recognize that antigen.”
The rapid test—officially known as the Sofia 2 SARS Antigen FIA …promises to “quickly detect fragments of proteins found on or within the virus by testing samples collected from the nasal cavity using swabs,” It can provide results within 15 minutes.
ANTIBODY tests, on the other hand, look for antibodies a person’s immune system has made in response to the virus—that helps doctors determine whether a person has previously been exposed to COVID-19.
“A positive antigen test reflects active infection, while a positive antibody test reflects recent or past infection“
Possibilities & Theories
“The COVID-19 PCR-Test – A Shot of Nanoparticles for Your Brain?” [14 Nov]:
Could it be, that the tips of the pcr test swabs contain nanoparticles, and when insterted deep through the nose to the the thin, sensitive, fragile cribriform plate (which is like an entry to the brain, perforated with fine holes), and when the long swab is turned, it depostis these near the brain? These holes are traversed by nerve cells (neurons) of the olfactory nerve.
“RNA vaccines offer many advantages. The physicians would not necessarily have to inject the vaccine. Most RNA vaccines are directly nasally administered. This seems to make sense, since many infections start in the upper mucous membranes“.
There are lots of links and references and some videos in this article, for example this: Johns Hopkins Researchers Engineer Tiny, Shape-Changing Machines That Deliver Medicine Efficiently to the GI Tract
“Inspired by a parasitic worm that digs its sharp teeth into its host’s intestines, Johns Hopkins researchers have designed tiny, star-shaped microdevices that can latch onto intestinal mucosa and release drugs into the body.”
Read on under: 6)
“What Effects Can These Nanoparticles Have in Your Brain?”
– end of article –